
Look
Look for swelling, redness, wounds or scars, sinuses - all with respect to the anatomical structures.
Feel
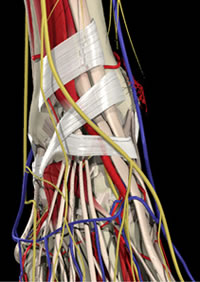
Lots of structures! The layers below will make it easier
Feel round the whole ankle, even the bits the patient is not complaining of. It may be worth leaving the most painful area to last, so that if the patient's compliance is then lost, you do not lose information on the rest of the ankle (and foot). Again, relate palpation to the areas the patient is complaining of and to the anatomical structures.
Move
Ask the patient to move the ankle through a full range of dorsiflexion/plantarflexion. Ask if any movement produces pain.
Remember that a significant proportion of dorsiflexion/plantarflexion occurs in the mid tarsal joint. Marking the foot as shown in the first video may help distinguish this.
Then move the ankle through the range of movement yourself. Use a hand under the foot to minimise mid foot movement so that the range you measure is likely to be the true range in the ankle. Again, ask if any movement produces pain. In particular, distinguish between mid-range pain, which is likely to be coming from the joint, and end-range pain, which may be due to impingement or set tissue contracture
Special tests
Special tests in this part of the ankle include
- anterior draw test
- varus tilt test
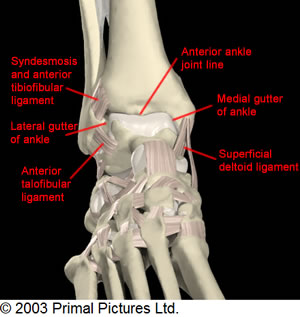
- external rotation test for syndesmotic pain
- Molloy-Bendall test for anterior impingement
Simple anterior draw test with ankle plantar flexed 20deg, pulling the calcaneum forward to draw the talus forward in the ankle mortise. Normal ankle should have minimal displacement and firm end-point
Alternative method (especially useful if you have small hands). Instead of drawing the ankle forward the foot is fixed and the tibia is pushed back. Unfortunately there is no data on the relative accuracy of these two methods.
Varus tilt test. The ankle is in neutral to lock the talus as much as possible. The calcaneum is tilted into varus to tilt the tibia. A finger on the lateral talus can help you judge how much tilt occurs. A normal ankle will have minimal tilt and a firm end-point.
The Molloy-Bendall test for anterior impingement (Molloy 2003). This tests for nipping of inflamed synovium between talus and tibia or fibula in maximum dorsiflexion. First check whether pain is produced at maximum dorsiflexion. If not, repeat the test with a finger in the joint line pressing the synovium into the joint. The test has a sensitivity of 95% and a specificity of 88% to predict the presence of synovitis
The external rotation test is the most accurate to predict syndesmotic instability. The ankle is held in neutral and the foot externally rotated to stress the syndesmosis. A positive test is the production of pain in the syndesmosis - the amount of actual instability is too small to feel.